
Posted November 29, 2018
“My life was a raging dumpster fire!” – Anonymous, after two weeks at a residential drug rehabilitation treatment center.
So, how does the practitioner or client engage in financial planning while the client is driven to desperately and surreptitiously feed their addiction or fearfully concede to a dependence on opiates? When abused, opiates morph into a swarm of locusts feeding on human capital. For an addict, or those individuals supporting the recovery efforts of an addict, human capital recovery starts by the client:
1) recognizing and acknowledging the reality of the client’s situation;
2) educating himself on options available for recovery;
3) determining a personalized course for recovery with the help of trusted personal and professional support systems;
4) Investing in himself by implementing a plan for recovery; and
5) pro-actively taking care of himself on an ongoing basis by attending therapy, living a healthy lifestyle, and rebuilding the parts of his life that may have been neglected during the darkest hours of dependence or addiction.
While developing a five-step plan may seem intuitive to some, there are challenges that must be acknowledged directly. Some of the challenges have to do with access to and affordability of treatment facilities, as well as the pharmaceutical industry’s and prescribing medical practitioners’ continued use of oxycodone. It is also important for patients to advocate for themselves—for their very own best interests from a position of power; knowledge is power.
Recent news, developments and perspectives…
The Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act, also known as the SUPPORT for Patients and Communities Act was signed into law on October 24, 2018. https://www.youtube.com/watch?v=2geQ0d3WsMY#action=share. This legislation is holistic in nature. It specifically addresses and provides guidance on opioid crisis issues such as Medicaid and Medicare provisions, detection and monitoring systems for synthetic opioids, behavioral health, opioid safety education, promotion of research to respond to the threat of the crisis itself, illicit drug importation, safe disposal of unused medication, treatment for veterans, support for grandparents caring for grandchildren, prescribing guidelines, support for mothers and care for infants suffering from neonatal abstinence syndrome and much, much more. See the text of the SUPPORT for Patients and Communities Act at the following link: https://www.congress.gov/bill/115th-congress/house-bill/6/text. The above list of areas covered by this Act is a mere fraction of the sweeping legislation.
The Drug Enforcement Agency (DEA) appears to be on the mission and engaged in the battle against illicit opioid distribution and prescribing practices. On November 15, 2018, Serio Juana Devoe was sentenced to 10 years in prison and eight years of supervision for attempting to distribute fentanyl and methamphetamines. The Anchorage Police Department and the Drug Enforcement Agency (DEA) cooperated on the case which was prosecuted as a result of the United States Department of Justice Project Safe Neighborhoods (PSN) program. PSN is a federally funded initiative that promotes nation-wide multi-agency efforts to reduce gun violence.[1],[2] On October 31, 2018, the acting administrator of the DEA Diversion Control Division, denied the DEA Certificate of Registration for Edward A. Ridgill, MD, effective immediately.[3] In August 2016, Dr. Ridgill was one of two doctors in Lynwood, CA that was arrested on federal drug charges for issuing prescriptions without a medical purpose. He issued more than 21,000 prescriptions for hydrocodone (Vicodin or Norco), codeine (for example, promethazine with codeine cough syrup, street name purple drank), alprazolam (Xanax), and carisoprodol (muscle relaxer). According to the investigation affidavits, there was evidence that the two doctors were large-scale suppliers for gang members.[4] In December 2017, Dr. Ridgill was convicted of 26 counts of unlawful distribution of controlled substances.[5]
The US Department of Health and Human Services maintains the National Practitioners Data Bank (NPDB). The NPDB was established by Congress in 1986 and serves as a web-based repository of reports and data that contain information on medical malpractice payments and adverse actions pertaining to health care professionals (practitioners, providers and suppliers). An analysis of the most recent data reveals that between 1990 and 2017, there were a total of 3848 DEA Adverse Action Reports and 635,125 state licensure adverse reports[6]. Below is a chart of the most relevant categories for the purposes of this report.
|
DEA Adverse Action Reports |
State Licensure Adverse Action Reports |
|
| Physicians, MD |
2699 |
4408 |
| Pharmacist |
0 |
1270 |
| Dentists |
341 |
1058 |
| Physicians, DO |
318 |
511 |
| Advanced Practice Nurses |
240 |
226 |
| Physician Assistants |
134 |
329 |
The below is a graphic representation of the number of reports issued each year for the specific practitioners listed in the table above. Clearly, the number of reports issued by the DEA and state licensing organizations on an annual basis significantly increased after 2008.
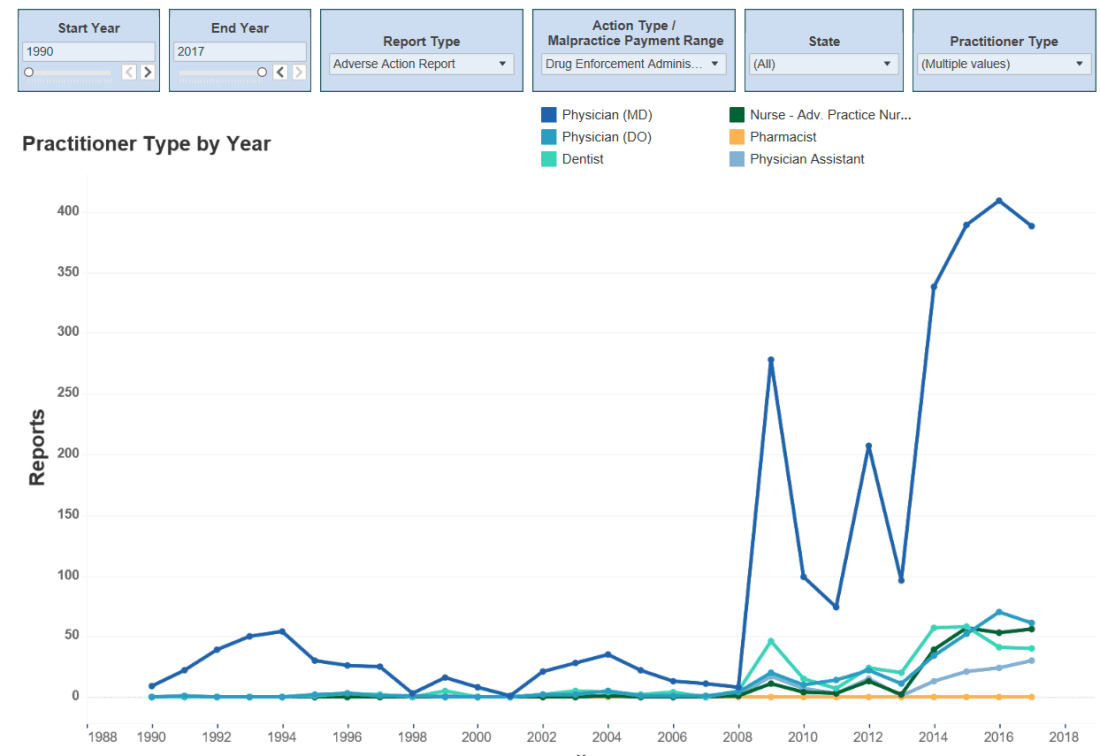 Number of DEA Adverse Action Reports; 1990 – 2017[7]
Number of DEA Adverse Action Reports; 1990 – 2017[7]
 Number of state licensure Adverse Action Reports; 1990-2017[8]
Number of state licensure Adverse Action Reports; 1990-2017[8]
In May 1986 the medical journal Pain published a research report by Drs. Russell K. Portenoy and Kathleen M. Foley entitled “Chronic Use of Opioid Analgesics in Non-malignant Pain: Report of 38 cases.” The doctors re-examined up to 7 years of data collected on 38 pain patients that were undergoing some form of opioid analgesic pain management for non-malignant conditions. After retroactively examining factors such as dosage, pain relief, toxicity, time in pain management therapy, and personality factors of 38 patients, Portenoy and Foley concluded “that opioid maintenance therapy can be a safe, salutary and more humane alternative to the options of surgery or no treatment in those patients with intractable non-malignant pain and no history of drug abuse.”[9] This study was used as the touchstone for the mass marketing of opioids as a go-to narcotic for pain relief…moderate to severe. As early as 1998, researches at the University of British Columbia in Vancouver published research that directly contradicted Purdue and FDA claims that OxyContin was safe to prescribe, in that there was a low probability that patients would become dependent on or addicted to the narcotic in a “time release” formulation. Purdue Pharma was aware of the research study published in the Journal of the Canadian Medical Association. The study revealed that on the streets of Vancouver, abusers learned to peel away the time release coating and crush the pills; they were called “peelers”, and one 30 milligram pill had a street value of $40. The very same pill sold for $1 at the pharmacy.[10] It is against this backdrop that some pharmaceutical companies, distributors and medical professionals claim that they have no responsibility for the current opioid contagion. Consider:
- Purdue Pharma has paid several hundreds of millions of dollars in government penalties and civil litigation over the last decade or so, however they are currently facing more than a thousand lawsuits brought by cities, states, and Native American tribes. In August 2018 the company hired restructuring lawyers in response to mounting law suits that claim several pharmaceutical companies mislead the public about the addictive nature of their opioid painkillers. The plaintiffs hope to recoup some of the costs of battling the epidemic. According to an October 2018 Wall Street Journal article, Purdue Pharma along with other drug manufacturers claim they did not cause the opioid crisis and want plaintiffs to show how the companies were to blame by presenting specific numbers of prescriptions and identifying specific residents (both data points in the hundreds) that were harmed by the opioid prescriptions.
- In a 2012 Wall Street Journal interview, Dr. Portenoy stated the following:
Did I teach about pain management, specifically about opioid therapy, in a way that reflects misinformation? Well, against the standards of 2012, I guess I did…We didn’t know then what we know now.
My patients are on very high doses, and I have patients who are executives in companies, hedge fund managers, hospital executives…I think that some of the literature that has emerged is not balanced…
What we are now dealing with in the United States is a movement of the pendulum back toward a level of concern and fear that is driving some policy decisions, that in my opinion, are very likely to harm the public health by reducing access to these essential drugs.[11], [12]
View the video-taped interview here: A Pain-Drug Champion Has Second Thoughts
- On November 2, 2018 the FDA approved Dsuvia (sufentanil), a synthetic opioid analgesic to be used in “acute pain settings”, such as emergency rooms and on the battlefields. It must be administered by a health professional in a “certified medically supervised healthcare setting”, not to be taken for more than 72 hours.[13] AcelRx Pharmaceuticals has approval to sell this opioid analgesic that is 10 times stronger than fentanyl and 500 to 1000 times stronger than morphine. The projected annual sales are $1.1 billion. [14]

“My life was a raging dumpster fire!” – Anonymous, after two weeks at a residential drug rehabilitation treatment center
The financial and human capital costs for treatment
The cost to treat substance abuse disorders is substantially less than the cost associated with battling the societal ills the abuse produces. Criminal justice, Neonatal Abstinence Syndrome, increased growth- rates and incidences of infectious diseases, injuries sustained while intoxicated and lost productivity are a few of the areas that increase the costs associated with the opioid epidemic. According to an article published in the Medical Care section of the American Public Health Association Journal, in 2013 only 3.6% of the $78 billion dollars spent on opioid use disorders in the United States was spent on treatment.[15] United States Department of Defense estimates for substance abuse treatment are as follows:
- $6552 per year for methadone treatment, including medication and integrated psychosocial and medical support services (assumes daily visits)
- $5980 per year for opioid treatment facilities that provide buprenorphine (includes medication and two meetings per week, stable patient)
- $14,112 per year for opioid treatment facilities that administer naltrexone and related services.
To place these expenditures in context, average annual expenditures for diabetes mellitus is $3560, and $5624 for kidney disease patients.[16] However, even more context is needed.
Residential substance abuse treatment programs that offer counseling, group therapy, psychological evaluations, medication, education about the addiction (remember, knowledge is power), psychosocial or behavioral interventions, family programs, relapse preventions programs, and sober housing referrals can be cost prohibitive for many of the would-be patients. The cost for these programs can be $15,000 to $30,000[17] per year…or higher. In accordance with the Affordable Care Act, mental health and substance abuse services are considered essential health benefits. It is important to review individual plans to determine the specifics of individual coverage, however pre-existing conditions are covered and there can be no annual or lifetime dollar limits on essential health benefits.[18] Some insurance companies will require patients to attend and fail an out-patient program before approving a holistic residential program. Therefore, even after the addict triumphs over the barriers of facing the reality that they are suffering from an opioid use disorder and facing the fear of giving up the pills and potentially suffering from chronic pain that has been dulled by the opioid use, there can be confusion about costs and which treatment options will be successful and affordable. Because the addiction is chronic, treatment and self-care in the form of individual and group therapy, medications (especially in the case of dual diagnosis treatment), healthy living, and measured, deliberate re-entry into the work place are critical and require structured processes. All of this adds up to ongoing costs that do not even address the financial burdens amassed by the nuclear and extended family in the forms of child support, divorces, lost capital assets and destroyed careers. The primary concern is to get better physically, emotionally, and psychologically…which means that finding work is not a primary concern, even in the face of the mounting financial burdens. For a period of time, the recovering addict will need to acknowledge and deliberately, where practical, tackle the realities of the dumpster fire that consumed jobs, family relationships, friendships, health and assets. Everyone touched by the addiction is in recovery.
Creating Peace Of Mind Waypoints and course corrections…
Consider integrating the following life planning waypoints into your overall financial planning process to help mitigate the risks associated with opioid dependency or addiction.
- Get CPR/Overdose training. Vice Admiral Jerome Adams, the U.S. surgeon general issued an advisory; In an April 2018 interview with NPR host Rachel Martin, he urged Americans to carry naloxone (commercial name Narcan), a medication to be administered in case of an opioid overdose. Not only do first responders carry the medication, households are encouraged to have the medication as part of home first aid kits. When asked why “ordinary Americans” should be prepared to use Narcan, he responded that “Over half of the overdoses that are occurring are occurring in homes, and so we want everyone to be armed to respond. We should think of it like an EpiPen or like doing CPR on someone.”[19] The Veterans Administration includes naloxone in defibrillator cabinets. A simple internet search reveals where you can purchase the medication without a prescription. Check your local pharmacy for an over-the-counter dose of this opioid overdose antidote. Emergency care is still necessary after an overdose, however if administered after oxycodone is injected or snorted, naloxone will counteract the effects of the opioid. As mentioned in previous posts, there are “good Samaritan” laws to protect individuals that administer naloxone and encourage vital medical attention after the medication is administered. Some states require school nurses to carry the antidote and many have used it; our high schools are the front line. Sadly, this is the new norm…be prepared.
- Proactively seek accountability when oxycodone is prescribed. Medical practitioners advise that it is important to manage pain after procedures that result in significant discomfort. In layman’s terms, patients can better tackle the healing process if they can follow post procedure directions for recovery without the distraction of pain that may make them hesitant to follow discharge directions. The law requires that patients complete specific documents acknowledging that they will receive oxycodone during recovery and that they understand how it will be prescribed, when it will be prescribed, under what conditions refills will be given, and what will happen if patients violate the contract pertaining to the use of the oxycodone narcotic. Show and discuss copies of the document you sign with at least one or two trusted friends or family members that will help during the recovery process. Ask about alternative pain medications. Federal guidelines, as of 2016, dictate that opioids be prescribed for no more than three to seven days.
- Know how to dispose of unused medication and do so immediately. Recently, Hollywood actress Jamie Lee Curtis revealed her struggle with opioid addiction; she became addicted after receiving a prescription for painkillers after plastic surgery. She admits to stealing pills from friends and family when she no longer had her own prescriptions re-filled. The U.S Food and Drug Administration website[20], [21] lists several options for disposal of used medicines, to include:
- National Prescription Drug Take-Back events – temporary medicine collection events; provide education on drug abuse. The Diversion Control Division section of the DEA website has a search tool; enter your zip code to find dates and times of local take back events.
- DEA registered collectors – safely and securely collect and dispose of pharmaceuticals containing controlled substances and other medicines. Locations can be retail pharmacies, hospital or clinic pharmacies, and law enforcement facilities or collection receptacles/drop boxes.
- Guidance on how to dispose of prescription medications that must be flushed immediately or disposed of in household trash.
- Get estate planning documents in order. Estate planning is not only for the wealthy. While estate planning primarily addresses ownership and transfer of assets, it is also about protecting family and determining a process for using assets as efficiently as possible before and after the estate owner’s death. Seek advice from an estate planning professional to address some of the potential human capital and financial issues that may arise as a result of opioid addiction, and the tools available to manage healthcare and assets. The documents below allow an individual to designate trusted “agents” to manage assets and medical decisions to varying degrees. These documents “starting points”, relevant in sickness and in health and part of a holistic planning processes. Once again, my premise is not that your financial trusted advisor or estate planning professional is a behavioral health professional; do not expect behavioral health advice.
- Power of attorney (POA) – Grants permission for someone else (an attorney in fact) to act on behalf of the principal (the person creating the POA). The attorney in fact can make legally binding decisions. The POA can include limitations on scope and length of time.
- Durable Power of Attorney (DPOA) – Similar to a POA, however, if the principal becomes incapacitated, the POA is no longer binding; DPOA remains in effect after the principal is incapacitated. In the event of incapacity, a trusted individual can be designated to manage assets and make financial decisions. If it is a “springing” DPOA it will become effective at the time of incapacitation. A durable power of attorney for healthcare (DPOAHC) is always “springing” and the scope is limited to medical decisions, not property decisions. A DPOAHC is not only appropriate for situations in which the principal might be terminally ill, but also if the principle is unable to give consent for medical procedures or decisions;
- Execute a plan for recovery. In general, any planning process includes: gathering information, analyzing the information, developing a process to reach clearly articulated goals, implementing the process with a sense of purpose, and remaining accountable by periodically measuring the rate and amount of progress toward the stated goals. Then start over. With recovery from opioid addiction, research shows that, in general, this process never ends. In his book Overcoming Opioid Addiction, author, Dr. Adam Bisaga provides a list of ways to earn “recovery capital” or a “build up of positives in life.” As a review, a suggested format for a way forward in the human capital recovery process for an addict, or those individuals supporting the recovery efforts of an addict are to:
- Recognize and acknowledge the reality of the opioid abuser’s situation;
- Seek education on options available for recovery;
- Determine a personalized course for recovery with the help of trusted personal and professional support systems;
- Invest in self by implementing a plan for recovery; and
- Pro-actively taking care of overall health on an ongoing basis by attending therapy, living a healthy lifestyle, and rebuilding the parts of the opioid abuser’s life that may have been neglected during the darkest hours of dependence or addiction.
As the recovery plan takes shape, consider integrating “recovery capital” in the following ways, which are listed in Dr. Bisaga’s book, which include, but are not limited to:
Participate in treatment and continuing care
Take advantage of therapy even if you have been doing well for a long time
Actively engage with a mutual self-help community
Encourage your partner and family to support your recovery
Support others in their recovery
Choose to live in an environment that is free of drugs
Finish education; find a stable and fulfilling job
Clear all past legal problems…and much more.[22]
Preemptive and proactive life and financial planning are tools that can be used to help overcome social and economic barriers to recovery. There are no guarantees but being prepared is a plus. The process for recovery is unique for each person, however it includes having an awareness of current developments and perspectives, quantifying the cost of medical treatment, and planning for successful redemption of human capital with the help of planning professionals and trusted personal advocates. The SUPPORT for Patients and Communities Act is comprehensive, law enforcement and licensing agencies are engaged, communities are developing educational programs and partnerships to save lives, and estate planning tools are available to assist in the planning process. A systemic problem requires comprehensive, innovative solutions. Not all are listed here. Everyone touched by the contagion is in recovery–all hands on deck to encourage and support our loved ones as they douse the “dumpster fires.”
–Terry
[1] Herraiz, Domingo S. “Project Safe Neighborhoods: America’s Network Against Gun Violence.” U.S. Department of Justice Office of Justice Programs Bureau of Justice Assistance, https://www.ncjrs.gov/pdffiles1/bja/205263.pdf, accessed on 11/24/2018.
[2] Underwood, Jodie. “Anchorage Man Sentenced for Fentanyl Trafficking” U.S Drug Enforcement Agency, https://www.dea.gov/press-releases/2018/11/15/anchorage-man-sentenced-fentanyl-trafficking , accessed on November 12, 2018
[3] US Department of Justice, Diversion Control Division, DEA Decision Order, https://www.deadiversion.usdoj.gov/fed_regs/actions/2018/fr1120_3.htm [Federal Register Volume 83, Number 224, Tuesday, November 20, 2018.
[4] Department of Justice, US Attorney’s Office Central District Of California, “Two Doctors Face Federal Charges of Illegally Writing Prescriptions for Addictive Narcotics Connected to Gang’s Drug Trafficking.” https://www.justice.gov/usao-cdca/pr/two-doctors-face-federal-charges-illegally-writing-prescriptions-addictive-narcotics. Augutst 29, 2016, accessed on 11/24/2018.
[5] https://www.deadiversion.usdoj.gov/fed_regs/actions/2018/fr1120_3.htm
[6] Singh, Harnam. National Practitioner Data Bank. Generated using the Data Analysis Tool at https://www.npdb.hrsa.gov/analysistool.
[7] Singh, Harnam. National Practitioner Data Bank. Generated using the Data Analysis Tool at https://www.npdb.hrsa.gov/analysistool.
[8] Singh, Harnam. National Practitioner Data Bank. Generated using the Data Analysis Tool at https://www.npdb.hrsa.gov/analysistool.
[9] Portenoy, R. K. and K. M. Foley, “Chronic Use of Opioid Analgesics in Non-malignant Pain: Report of 38 Cases.” Pain, May 1986, https://www.ncbi.nlm.nih.gov/pubmed/2873550, accessed on 11/24/2018.
[10] Sajan MD, Amin, Trevor Corneil, MD and Stefan Grzybowski, MD, MClS. “The Street Value of Prescription Drugs,” from the Department of Family Practice, University of British Columbia, Vancouver, BC , CMAJ 1998, volume 159, pgs. 139-42 . www.cmaj.ca/content/cmaj/159/2/139.full.pdf, accessed on 11/24/2018.
[11] Catan, Thomas and Evan Perez. “A Pain-Drug Champion has Second Thoughts.” Wall Street Journal, Dec 15 2012, Eastern edition ed. ProQuest. 11/25/2018, accessed on 11/24/2018.
[12] Catan, Thomas and Evan Perez
[13] “Dsuvia Approval History.” Drugs.com, reviewed by J. Stewart on 11/13/2018. https://www.drugs.com/history/dsuvia.html, accessed on 11/25/2018.
[14] “FDA Approved new Opioid Drug Called Dsuvia.” https://abcnews.go.com/GMA/Wellness/video/fda-approved-opioid-drug-called-dsuvia-58940799, 11/3/2014, accessed on 11/13/2014.
[15] Florence CS, Zhou C, Luo F, Xu L. “The Economic Burden of Prescription Opioid Overdose, Abuse, and Dependence in the United States.” Med Care. 2016;54(10):901-906. doi:10.1097/MLR.0000000000000625. Accessed 11/13/2018.
[16] “Medications to Treat Opioid Use Disorder.” National Institute on Drug Abuse, https://www.drugabuse.gov/publications/research-reports/medications-to-treat-opioid-addiction/how-much-does-opioid-treatment-cost, accessed 11/24/2018.
[17] Adam Bisaga, MD, Overcoming Opioid Addiction, (New York: The Experiment, LLC, 2018) 177.
[18] “Mental Health and Substance Abuse Coverage.” Healthcare.gov, https://www.healthcare.gov/coverage/mental-health-substance-abuse-coverage/, accessed on 11/27/2018.
[19] “Surgeon General Urges More Americans to Carry Opioid Antidote.” Soundbite of Sleep Dealers “The Way Home,” NPR Morning Edition, hosted by Rachel Martin, 4/5/2018. https://www.npr.org/templates/transcript/transcript.php?storyId=599538089, accessed on 11/24/2018.
[20] “Disposal of Unused Medicines: What You Should Know.” U. S. Food and Drug Administration. https://www.fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsingMedicineSafely/EnsuringSafeUseofMedicine/SafeDisposalofMedicines/ucm186187.htm, accessed on 11/25/2018.
[21]“Prescription Drug Take Back Day.” US Drug Enforcement Agency Diversion Division, https://www.deadiversion.usdoj.gov/drug_disposal/takeback/index.html, accessed on 11/27/2018.
[22] Bisaga 208.
